










Background
Aortic stenosis (AS) is the most common primary heart valve pathology, with a growing prevalence in the Western world because of an ageing population.1 Prognosis, if the condition is untreated, is poor and registry data have shown significant mortality in patients on waiting lists for aortic valve intervention.2 As a result, healthcare systems around the world are under increasing pressure to deliver timely treatment for severe AS.
Transcatheter aortic valve implantation (TAVI) has revolutionised the treatment of severe, symptomatic AS by enabling the treatment of older patients who are ineligible for surgical aortic valve replacement (SAVR) with a less invasive, but equally effective, therapy.3 Subsequent randomised controlled trials have established TAVI as non-inferior to SAVR even in younger and lower surgical risk patients.4,5 These findings have been incorporated into recent international guidelines, broadening the indication for TAVI. Demand is likely to continue growing, with on-going studies exploring additional novel indications, which will potentially add new cohorts of patients who require treatment.6–8
The number of TAVI procedures undertaken in the UK has grown year on year since the first procedure was performed in 2007, such that the annual volume of TAVI now exceeds that for SAVR.9 Despite this, the number of TAVI procedures undertaken relative to population in the UK is well below that of almost all other Western European nations. In 2019, 93 TAVI procedures were performed in the UK per million population (pmp). This represented just over two-thirds the average in western Europe (141 pmp), and approximately one-third of that in Germany (292 pmp).10 Delays to diagnosis and treatment caused by the COVID-19 pandemic have only served to exacerbate the problem of access to TAVI and SAVR, resulting in a substantial backlog of patients with severe, symptomatic AS in need of treatment.
As well as the low overall numbers of TAVI relative to the population, there is substantial geographical variation within the UK for the delivery of treatment. Specifically, we have previously highlighted an 11-fold variation in TAVI rates pmp across the different clinical commissioning groups (CCGs).11 However, that analysis did not account for the total number of aortic valve interventions, inclusive of SAVR. It is possible that some regions with lower rates of TAVI pmp compensate with higher rates of SAVR.
The aim of the present study is to use data from the UK TAVI registry and the National Adult Cardiac Surgery Audit (NACSA) to assess the overall volume of aortic valve intervention in England, and to provide an updated and more nuanced description of the geographical variation in access to TAVI and SAVR across the country.
Methods
Transcatheter Aortic Valve Implantation Data
We obtained data on all TAVI procedures performed between 1 April 2019 and 31 March 2023 from the UK TAVI registry.12 The registry is managed by the National Institute of Cardiovascular Outcomes Research (NICOR) and captures the baseline characteristics and procedural details from all UK hospitals that perform TAVI.13 Regional data based on CCG are only available for England, so our analysis is restricted to the 36 hospitals that undertake TAVI in England. The data are presented as TAVI procedures pmp, and patients are matched to CCGs based on the postcode of their residence, rather than where the procedure was carried out.
Surgical Aortic Valve Replacement Data
The NACSA database, from which the SAVR data for this analysis were extracted, is also managed by NICOR, and includes data on all adult SAVR cases in the UK.14 To allow comparison with TAVI rates, SAVR volumes are presented pmp and patients are again matched to CCGs based on their residential postcode. For the purpose of this analysis, only isolated SAVR performed for severe AS between 2019 and 2023 were included. Combined SAVR and coronary artery bypass graft (CABG) cases were excluded on the basis that coronary artery disease may have been the primary indication for surgery, with SAVR undertaken for treatment of bystander aortic valve disease.
Dispersion of the rates of TAVI and SAVR across CCGs is reported pmp with medians and interquartile ranges (IQRs). Geographical variation between CCGs was assessed using rates pmp and the relationship between TAVI and SAVR rates was determined using the Pearson correlation coefficient.
Results
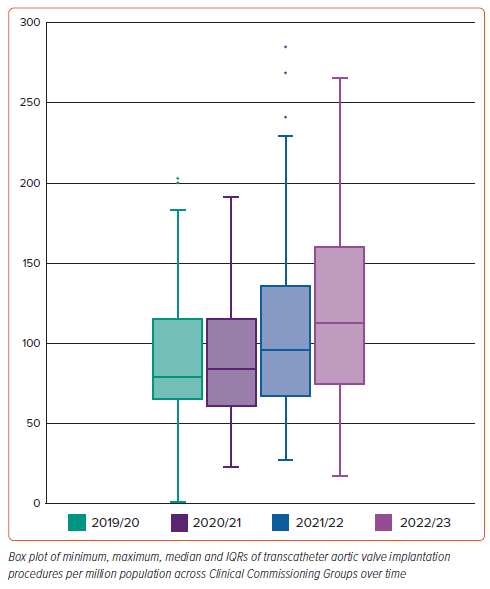
In 2022/23, 7,697 TAVI procedures were performed in England, with an overall rate of 136 pmp. This followed an annual increase in TAVI volume of 3% from 2019/20 to 2020/1, over 20% from 2020/21 to 2021/22 and a further 15% from 2021/22 to 2022/23.
The increase in the median TAVI rates pmp by CCG from 79 in 2019/20 to 112 in 2022/23 was accompanied by a more striking increase in the interquartile ranges (IQR 66–115 in 2019/20 and IQR 76–159 in 2022/3), thus demonstrating that the observed increase in the overall rates of TAVI over time was associated with widening of the geographical variation in access to the procedure across England (Figure 1).
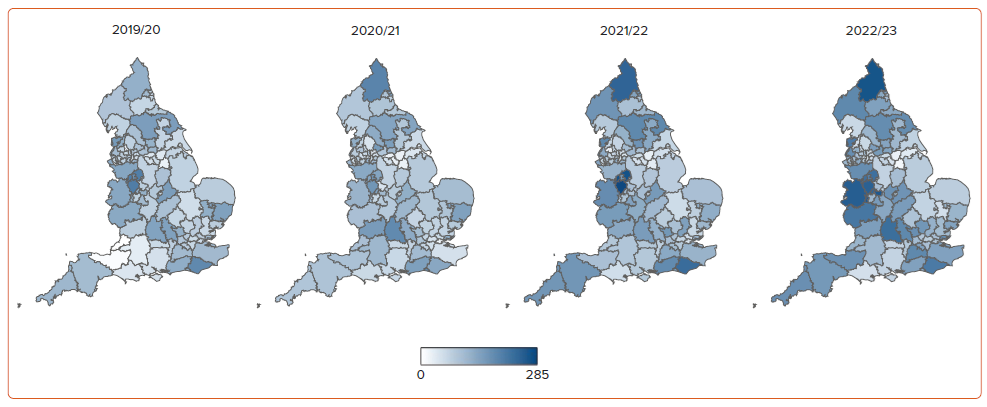
In 2022/23, there was a more than 15-fold variation in TAVI rate pmp by CCG. The disparities in the delivery of TAVI service across the country between 2019 and 2023 are illustrated in Figure 2.
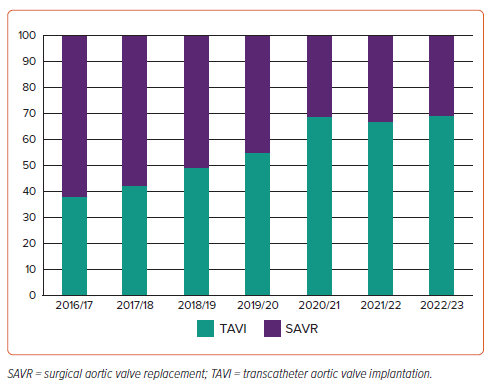
The volume of isolated SAVRs performed in England declined between 2016 and 2023 in parallel with the observed increase in the overall numbers of TAVI (Figure 3). In the year 2022/23, 3,396 isolated SAVRs were undertaken, with an overall rate of 60 pmp and a TAVI:SAVR ratio of 2.3 in England with ratios ranging from 0.2–6.8 across different CCGs as shown in Supplementary Figure 1.
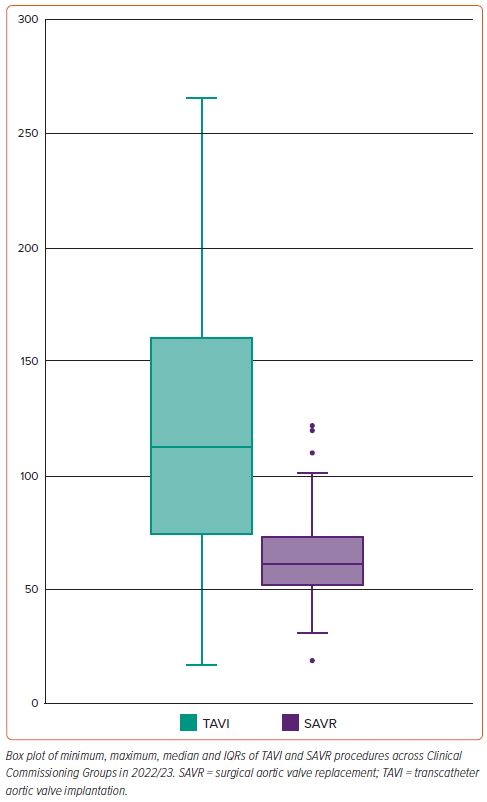
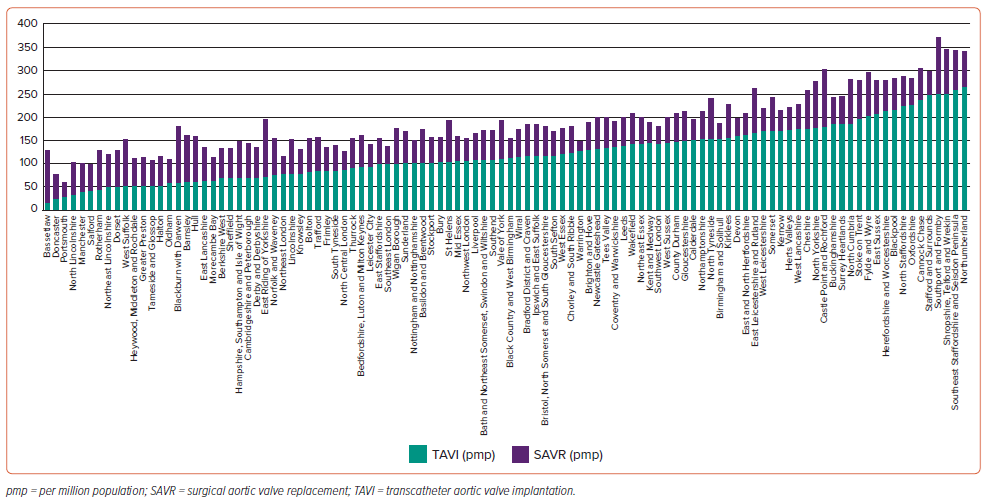
As with TAVI, substantial regional variation was observed in SAVR numbers across England, with SAVR rates ranging from 19 to 123 pmp in 2022/23. The median number of SAVRs performed pmp across all CCGs was 61.5 (IQR 52–72.8) in the same year. However, the magnitude of the variation in SAVR across the different CCGs in England was substantially smaller than that seen in TAVI, with an overall 6.5-fold variation in SAVR rate pmp between CCGs, compared with the 15-fold variation seen for TAVI. Figure 4 illustrates the medians and IQRs of both TAVI and SAVR rates pmp in all CCGs in England in 2022/23.
When combining the rates of TAVI and SAVR across individual CCGs in England, there appears to be a more than sixfold variation in access to severe AS treatment, with a median of 176 (IQR 144–213) as shown in Figure 5. Notably, there is no clear relationship between the rates of TAVI and these for SAVR pmp in England, with a correlation coefficient of 0.06. In addition, regions with low rates of TAVI do not appear to have higher rates of SAVR (Figure 5).
Discussion
We analysed data from the UK TAVI registry and National Adult Cardiac Surgical Audit to evaluate geographical inequality in access to aortic valve intervention for severe aortic stenosis in England. There are four principal findings. First, TAVI volume has increased over time in England, now exceeding that of isolated SAVR, given a simultaneous progressive fall in isolated SAVR procedures. Second, the geographical variation in access to TAVI across England remains substantial, with no reduction in heterogeneity over time. Third, geographical variation in access to SAVR is evident, but is less profound than that for TAVI. Fourth, there is no relationship between the rates of TAVI and those of SAVR across individual CCGs, meaning there is a marked geographical inequality in access to any form of intervention for severe AS.
Overall, these data demonstrate substantial heterogeneity in access to aortic valve interventions in England, with under-use of TAVI and SAVR in multiple areas of the country. Analysis of UK TAVI services has demonstrated that long waiting lists for TAVI result in over 500 avoidable deaths annually.11
Despite the increase in TAVI volume in England to 136 procedures pmp in 2022/3, numbers remain below comparable countries.9 In Western Europe and the US the rates of TAVI pmp were 141 and 176, respectively, in 2019, and will likely have increased substantially since.10,15 The burden of untreated severe AS is already high in the UK and is estimated to grow over the coming years.16,17 Furthermore, untreated severe symptomatic AS has a poor prognosis, with 50% mortality at 2 years.18
The COVID-19 pandemic has further increased the pressure on aortic valve interventions as elective cardiac surgery was suspended to reserve intensive care capacity. A recent report suggests that an increased use of TAVI is needed to reduce the NHS backlog and waiting list deaths in the post-COVID-19 era.19 In reality, our study demonstrates that contemporary provision of TAVI in England remains inadequate even before this factor is taken into account, and service expansion is needed to tackle current and future needs.
Compounding the fact that provision of TAVI in the UK is low compared with similar developed nations, the extent of geographical inequality within England is of concern. Specifically, a more than 10-fold variation in TAVI rate pmp within a single healthcare system implies a need for levelling up to ensure adequate provision of therapy to the whole population. We identified 10 CCGs with a TAVI rate below 50 pmp, and a further 20 CCGs with rates below 75 pmp; at the other end of the spectrum 22 CCGs perform more than 150 TAVI procedures pmp. Importantly, we have illustrated in this study that this postcode variability has remained unchanged over the last 3 years.
While our analysis of isolated SAVR also shows geographical variation in access to surgical intervention, these differences are less marked compared with TAVI. There is also no relationship between SAVR and TAVI rates pmp across the different CCGs, therefore showing that low rates of TAVI are not compensated for by higher SAVR rates.
Our findings highlight an urgent need to improve access to treatment for aortic stenosis across the UK, but – particularly – to target those parts of the country where provision appears inadequate. The first step is to highlight the inequality by sharing data with the key stakeholders, namely TAVI and SAVR centres, integrated care boards (ICBs) that are responsible for local commissioning, regional and national specialist services commissioners and patient groups. In addition, a multi-faceted national action plan to address the under-provision and inequality of aortic valve intervention is recommended as follows:
- Annual reports of TAVI and SAVR activity by locality should continue to be provided through the National Cardiac Audit Programme, with a focus on geographic heterogeneity so that this can be tracked and addressed year-on-year.
- ICBs need to be mandated to address the under-provision where it is identified.
- National professional societies, specifically the British Cardiovascular Society, British Cardiovascular Intervention Society and Society for Cardiothoracic Surgeons should be responsible for educational programmes to inform best practice in pathways of rapid assessment and treatment of patients with severe AS.20
- Formalised valve networks should be developed across integrated care systems, facilitating connection of district hospitals and cardiac surgical centres and implementation of a single referral pathway for AS regardless of the destination treatment.21
- Benchmarking standards and quality indicators should be implemented, with public reporting of performance against these standards in individual centres.11,22
- A fast-track pathway for severe AS should be introduced, equivalent to that in place for cancer, with definitive treatment by TAVI or SAVR within 8 weeks of referral.
Our study has highlighted important and unacceptable under-provision with geographical variation in TAVI services in England. It raises issues that demand a thorough review of the current care pathways for these patients, including the need to increase capacity for growing demand for aortic valve intervention in existing centres, while also considering whether new, non-surgical TAVI centres may be required in some areas. Given the avoidable mortality involved, these service reviews should be performed with some urgency.
Study Limitations
This study has some important limitations. Only isolated SAVR was included in this analysis, whereas SAVR with CABG was not. While this will have resulted in an under-estimation of the overall rates of SAVR for severe AS, it is unlikely to impact the key findings of our study, in particular the relative use of TAVI and SAVR in different CCGs. Many patients undergoing combined SAVR and CABG would have coronary artery disease as the primary indication for surgery with bystander moderate or severe AS or even aortic regurgitation.
In addition, we could not investigate whether some of the variation in TAVI numbers between regions might reflect differences in patient demographics that could imply variation in the prevalence of severe AS. However, it is unlikely that such differences could explain the magnitude of the observed geographical variation.
Conclusion
The overall rate of TAVI in England remains well below that seen in other developed countries. Substantial geographical heterogeneity in access to TAVI exists, with no improvement over recent years. Under-provision of TAVI in many areas is not compensated for by higher rates of SAVR, indicating an overall under-provision in the treatment of severe AS. There is an urgent need to increase capacity for AS treatments and to focus efforts on those regions where current provision is inadequate.
Clinical Perspective
- Reports from the UK Transcatheter Aortic Valve Implantation (TAVI) registry have shown that TAVI rates in the UK are below the average for western Europe, with substantial geographical variation in the delivery of TAVI care.
- However, the relationship between TAVI rates and those for surgical aortic valve replacement (SAVR) across individual clinical commissioning groups has not previously been explored.
- This paper provides contemporary data from the UK TAVI registry and the National Adult Cardiac Surgery Audit.
- We highlight that access to TAVI remains heterogeneous and that regions with low TAVI rates do not compensate with higher rates of SAVR.